
Diagnosis of Behçet’s Disease
Diagnosis of Behçet’s disease can be challenging because there is no single test that confirms it. Instead, doctors rely on a combination of clinical criteria, patient history, and exclusion of other conditions. The process often involves multiple specialists, including dermatologists, rheumatologists, and ophthalmologists.
Diagnostic criteria often include:
- Recurrent oral ulcers
- At least three episodes in one year is a key requirement.
- These ulcers are usually painful, shallow, and similar to canker sores.
- At least two of the following:
- Recurrent genital ulcers (painful and scarring)
- Eye inflammation (uveitis or retinal vasculitis)
- Skin lesions (acne-like or nodular rashes)
- Positive pathergy test: Skin overreacts to a minor prick, forming a red bump or ulcer
- Other possible symptoms:
- Joint pain or swelling
- Gastrointestinal inflammation
- Brain involvement (neurological Behçet’s)
- Blood clots or aneurysms
Tests used to support diagnosis include:
- Blood tests: Rule out infections or other autoimmune diseases
- Eye examination: Detect inflammation of the retina or uvea
- Biopsy: In rare cases, tissue samples may help distinguish Behçet’s from similar conditions
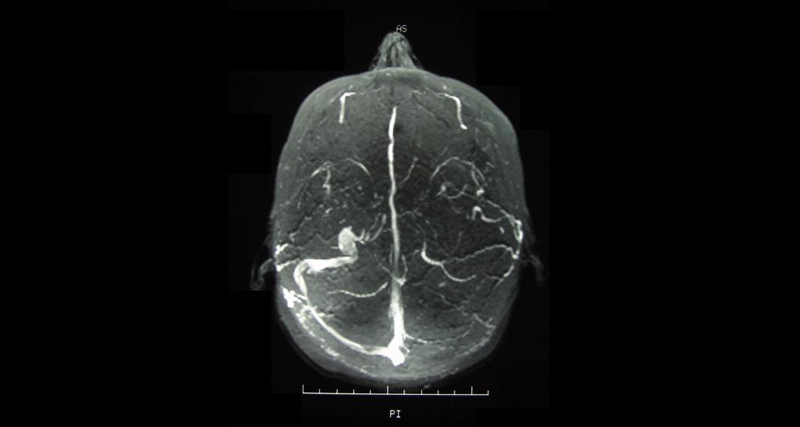
- MRI or CT scans: For neurological or vascular symptoms
The pathergy test (common in countries where Behçet’s is prevalent) is less reliable in South Africa and other regions where the disease is rarer.
Because the symptoms can appear years apart and mimic other illnesses, Behçet’s is often misdiagnosed. In South Africa, people may initially be treated for STIs, oral herpes, or inflammatory bowel disease before the full pattern is recognised.
Diagnosis of Behçet’s Disease
The earlier the diagnosis, the better. Regular monitoring and multidisciplinary care are essential to track the disease’s progression and avoid complications such as blindness or blood vessel rupture.
👉 [Next: Treatment and Management of Behçet’s Disease]